How to win the fight against conversion practices in Europe

Activists across Europe are working to end conversion practices, but the insidious and underground methods out there of trying to change a person’s sexual orientation or gender identity make for a battle against many odds.
At the ILGA-Europe offices we recently hosted a meeting with activists from different parts of Europe to discuss the way forward for working to end conversion practices. For this blog, we sat down with some of them to discuss the complexities involved.
One of the key messages that emerged from the discussion was the need to expand the public’s understanding of conversion practices. While many still associate these practices with extreme forms of torture – such as electroshock therapy – the reality is more subtle. Conversion practices often take covert forms that still cause significant harm.
“Conversion practices might not always look like torture, but the effect of them is the same,” Erin Lux from Equality Scotland explained. “It is a process of trying to change or suppress who a person fundamentally is.” Curro Peña Díaz from No Es Terapia added, “What we think of as conversion practices – violent therapies – are often much more subtle and insidious. They can appear helpful, but they’re actually harmful.”
The covert nature of these practices makes them difficult to identify and combat. As Parvy Palmou from The Greek Transgender Support Association pointed out, “Most conversion practices are done behind closed doors, making them hard to prove.” Thomas Ologo from Inter-LGBT in France echoed this, noting that many conversion therapies have gone underground. He also emphasised the need for continued education, saying, “We need to ensure that people – especially professionals – understand the nuances of conversion practices so they can help prevent them.”
This shows the importance of shifting the conversation to understand that conversion practices are still widespread.
Do conversion practice bans work?
Many activists agree that while a ban on conversion practices is a necessary starting point, it is not enough. In countries where bans exist, these practices still occur underground. Aksel Emil Houmann from LGBT+ Denmark said, “A ban is not enough. We need to change the belief that queer people are broken.”
Parvy Palmou also pointed out the limitation of bans, particularly in Greece, where conversion practices are banned for minors but not for adults because adults have the capacity to provide consent. “Can someone truly consent to the torture of their own identity?” she questioned.
“By collaborating with other groups, like children’s or women’s organisations, we become stronger and more effective.”
Askel Emil Houmann, LGBT+ Denmark
For bans to be effective, they need enforcement, public awareness, and comprehensive support systems. Erin stressed: “We need to raise awareness so people understand that conversion practices are still happening and that we can stop them through both legislation and support services.”
Activists also highlight the importance of working with a broad coalition of allies. Aksel added, “By collaborating with other groups, like children’s or women’s organisations, we become stronger and more effective.”
Not simply passing laws
Alongside legal measures, activists emphasise the need to protect victims and change public attitudes. According to Curro Peña Díaz: “We need protective measures to empower victims and help them escape these harmful practices.”
Rosario Coco from Gaynet in Italy highlighted the importance of education: “We need to reach all stakeholders – mental health professionals, human rights organisations – because conversion practices involve many actors.”
Ultimately, the fight is not just about passing laws, but about shifting societal attitudes. Rosario pointed out, “A ban is crucial, but we must also move public opinion, influence institutions, and educate civil society.”
The fight to end conversion practices is complex but not impossible. Activists across Europe are leading the charge, with strategies that include raising awareness, enforcing legislation, building coalitions, and changing public perceptions. As Curro Peña Díaz summed up: “We need to ensure people know conversion therapy is still happening and that it’s extremely harmful.”
Joint statement on the decision to ban puberty blockers for trans youth in the UK
The recent decision to indefinitely ban the private prescription of puberty blockers for trans youth in the UK marks a profoundly troubling development in the ongoing struggle for the rights of trans people and access to necessary, life-saving and evidence-based healthcare.
In the UK, where no form of trans-specific healthcare is currently available for minors through the NHS and waiting lists have reached six years, the government’s decision to ban the private prescription of puberty blockers for trans youth constitutes a de facto ban on puberty blockers. This decision, which overrides years of established medical guidance and expertise, is deeply political, rooted in a divisive public discourse and misinformation rather than the recommendations of leading medical authorities. It threatens the well-being of vulnerable trans youth, whose lives depend on timely, supportive, and individualised healthcare.
ILGA-Europe, IPPF European Network, TGEU, IGLYO, and The Kite Trust call on the UK government to reconsider this harmful decision and to engage meaningfully with both the medical and scientific community and civil society groups representing the interests of trans youth and trans adults.
The framing and justification for this ban have leaned heavily on a polarised and often misleading public narrative about trans identities and related trans healthcare and epistemologically, and methodologically questionable studies about trans identities and trans-specific healthcare. Despite claims of prioritising child safety, this decision disregards the consensus of medical professionals and organisations such as the World Professional Association for Transgender Health (WPATH) and the Endocrine Society’s Clinical Practice Guideline, which have long endorsed puberty blockers as a safe and reversible option for managing gender dysphoria in minors. These treatments allow young people experiencing distress with their assigned gender to pause puberty, giving them time to better understand their needs and identity, without the added pressure of physical changes brought on by puberty.[1]
The political instrumentalisation of healthcare for trans minors has become a rallying point for anti-trans rhetoric, which often conflates all trans-specific healthcare with irreversible medical interventions. This characterisation is not only inaccurate but also deeply harmful. Puberty blockers do not lead to permanent medical transition[2] – they are a widely used and reversible treatment prescribed for various conditions, including precocious puberty.[3] By banning them for trans youth specifically, the UK government is singling out a vulnerable group for discriminatory and harmful treatment based on ideology rather than evidence.
Misinformation about the nature and effects of puberty blockers has played a significant role in shaping public opinion and policy. Opponents of trans-specific healthcare frequently cite exaggerated or unfounded claims about the risks of these treatments, ignoring the robust body of research demonstrating their safety and efficacy. Long-term studies show that puberty blockers and other trans-specific healthcare significantly reduce rates of depression and suicidality among trans youth[4] —outcomes that align with broader understandings of the critical importance of affirming care for marginalised populations.
Expert voices, including paediatric endocrinologists, psychologists, and trans health specialists, have been sidelined in favour of rhetoric that frames trans-specific healthcare as controversial. This erasure of medical expertise undermines the principles of patient-centred care and puts the health of trans youth at risk. The decision to ban puberty blockers ignores the individualised, case-by-case assessments that qualified professionals conduct before prescribing such treatments,[5] opting instead for an unyielding prohibition that strips both doctors and families of agency.
The consequences of this ban will be devastating. For many trans youth, the ability to access puberty blockers represents a lifeline. Denying them this care will force young people to undergo the changes of puberty associated with their assigned gender, exacerbating gender dysphoria and increasing risks of mental health struggles, including anxiety, depression, and suicidal tendencies. By removing a critical tool for early intervention, this decision condemns trans youth to unnecessary suffering and places an already marginalised group at greater risk of harm. Furthermore, this policy undermines the trust between trans individuals and the healthcare system. Families seeking support for their children will face increased barriers, uncertainty, and stigma, while healthcare providers may find themselves unable to offer the care they know to be best for their patients. These ripple effects extend beyond trans youth, chilling the broader provision of trans-specific healthcare and reinforcing a climate of fear and hostility.
Trans children and young people deserve safety, understanding, and access to the same standard of care afforded to their peers. Decisions about their healthcare should be guided by medical evidence and the expertise of trained professionals, not by political agendas. The indefinite ban on puberty blockers represents a failure to prioritise the rights and well-being of trans youth, and it sets a dangerous precedent for further erosion of the rights of LGBTI persons in the UK.
We urge policymakers to reconsider this harmful decision and to engage meaningfully with both the medical and scientific community and civil society groups representing the interests of trans youth and trans adults. Upholding the dignity and humanity of trans youth requires a commitment to evidence-based healthcare, free from the distortions of ideology and misinformation. Only by centering the voices and needs of trans youth can we hope to build a society that values and protects all its members.
Signatories
- ILGA-Europe
- IPPF European Network
- TGEU
- IGLYO
- The Kite Trust
[1] Cal Horton, Experiences of puberty and puberty blockers: Insights from trans children, trans adolescents, and their parents, Vol. 39(1), Journal of Adolescent Research, available at: https://journals.sagepub.com/doi/full/10.1177/07435584221100591v.
[2] Hannema et al, Endocrine management of transgender and gender diverse adolescents: expert opinion of the ESPE Working Group on Gender Incongruence and the Endo-ERN main thematic group on Sexual Development and Maturation, available at: https://pubmed.ncbi.nlm.nih.gov/39622214/.
[3] Giordano & Holm, Is puberty
delaying treatment ‘experimental treatment’?, Vol 21(2) International Journal of Transgender Health (2020).
[4] Van der Miesen et al, Psychological Functioning in Transgender Adolescents Before and After Gender-Affirmative Care Compared with Cisgender General Population Peers, Vol 66(6) Journal of Adolescent Health (2020); Olson et al, Mental Health of Transgender Children Who Are Supported in Their Identities, Vol 137(3) Pediatrics (2016); Nath, R., Matthews, D.D., DeChants, J.P., Hobaica, S., Clark, C.M., Taylor, A.B., Muñoz, G. (2024). 2024 U.S. National Survey on the Mental Health of LGBTQ+ Young People. West Hollywood, California: The Trevor Project. www.thetrevorproject.org/survey-2024.
[5] Cass, Hilary (2024), Independent review of gender identity services for children and young people: Final report, pp. 168-169, available at: https://cass.independent-review.uk/home/publications/final-report/
New regulations pose greater risks to trans people in Turkey

New changes from the Turkish authorities to the accessibility of hormones for trans people further threaten health and lives
On 20 November, the Turkish Medicines and Medical Devices Agency announced a new regulation that requires an e-prescription to access certain hormones used by trans people. The restrictions regulate access to hormones used mainly by trans masculine people as well as hormones used to treat diabetes. The two hormones under this new regulation used by trans women are also the same hormones used by cis women for birth control. This regulation therefore not only impacts trans people but also cis women and people with diabetes.
The new regulation exposes the pre-existing inadequacies in access of trans persons to healthcare services. While the regulation can be seen as an attempt to regularise the process of distribution and use of hormones, making the procurement and treatment safer for users, the Turkish healthcare system is extremely inaccessible for trans people, in particular as regards trans-specific healthcare. As a result, this new regulation will have severe consequences for trans people.
Currently in Turkey university research hospitals are the only hospitals that have specific gender transition councils which assess and provide a medical report for trans persons, which doctors then use to prescribe the necessary hormones. However, these hospitals are only available in 13 of the 81 provinces (usually those with major cities), resulting in those trans people living in rural areas having to travel to one of these 13 provinces. The journey time is usually long, and appointment availability is scarce, making such trips less affordable and accessible. For those who already live in major cities, it is still difficult to access the healthcare system as appointments are rarely available due to high demand – it can take several months to secure a first appointment. Subsequent appointments also have a similar waiting time. In total, it takes a minimum of six months to receive the necessary report for accessing hormone prescriptions. It is time and resource-intensive, and transphobia is often encountered along the way.
Hormones are a key part of trans-specific healthcare for many trans people – they impact not only physical traits but also frequently psychiatric health and wellbeing. For trans persons who have had their gonads removed, hormones are critical for good physical health, as stopping hormone therapy can lead to osteoporosis, among other things.
As a result, this new regulation will have severe negative consequences for the healthcare and mental health of trans people across Turkey, in particular trans masculine people and trans people in poverty. Many trans people will no longer be able to access these hormones, and some will even turn to unregulated pathways to procure them, which can result in health risks and exorbitant prices.
For such a prescription regulation to produce positive effects, the Turkish healthcare system needs to be restructured in such a way as to ensure that trans people can access healthcare in hospitals in all areas of the country. Trans-specific healthcare needs to be more widely provided and understood so that the current high demand can be met, with medical professionals ensuring the right to health of each patient, without discrimination.
More broadly, Turkey should uphold the case law of the European Court of Human Rights on legal gender recognition under Article 8. It should introduce a new legal framework that is quick, transparent and accessible with no requirements for invasive surgeries, and wide access to trans-specific healthcare. It should comply with the World Health Organisation’s 11th revision of the International Classification of Diseases which depathologises trans people in all areas of life.
Recent incidents of limitations on the right to freedom of assembly for LGBTI people in Turkey
On 20 November police blocked a demonstration to commemorate victims of transphobic violence in Ankara on the International Trans Day of Remembrance, and arrested four people, including a member of the Ankara Bar Assocation.
On 23 November police intervened in a demonstration by trans activists in Istanbul against the new e-prescription regulation, detaining 38 people. They were released after providing statements to the police.
On 25 November – The International Day for the Elimination of Violence Against Women – hundreds of people took to the streets in cities across the country, and were met with police repression in many cases. In particular, in Istanbul, the Governor’s Office banned all protests and demonstrations on the specified date, and police interventions resulted in 169 arrests. All of those arrested have since been released, apart from two LGBTI+ people from Azerbaijan, who were taken to repatriation centres. Due to the severe conditions and ill-treatment they were subjected to, including being deprived of food and medications, they were forced to “voluntarily return” to Azerbaijan. One of them was an LGBTI+ human rights defender from Azerbaijan who immigrated to Turkey due to being at risk of arrest in their country.
In Turkey LGBTI+ people are regularly subjected to arbitrary detention (often with excessive police force) and charged for participating in public events, or for holding rainbow flags in the public space. Public demonstrations are frequently banned or postponed under the pretext of “national security”, “public order”, “prevention of crime”, “protection of public health” or “public morals”, with police and governors excessive powers. These practices which include vague limitations on public assemblies allowing for arbitrary interpretation, breach Turkey’s own Constitution (Article 34) and the European Convention on Human Rights (Article 11) to which Turkey is party. Turkey should bring its practices in line with the ECHR and its own Constitution, halting arbitrary banning of protests and detention of participants.
World Aids Day 2024: Making a world where HIV is history

Although it seems a long way off, HIV activists believe that consigning HIV and AIDS to history is an achievable goal. This World AIDS Day, we explore how that goal might become a reality.
World AIDS Day is an opportunity to reflect on the progress made in the fight against HIV, honour those we’ve lost, and recommit to creating a world where HIV is no longer a source of stigma, discrimination, or inequality.
As Paul Wickson, a queer activist from the UK, shares in his powerful statement:
“I lived through the HIV and AIDS crisis of the 80s and 90s. I lost friends to the disease, like so many millions of others… I want to see a world where HIV is history.”
HIV activism, like Paul’s, has brought us closer to that vision, but much work remains. Today, with advances like Undetectable = Untransmittable (U=U) and PrEP, people living with HIV can lead healthy, fulfilling lives. Yet, stigma and barriers to accessing testing and treatment persist, disproportionately affecting LGBTI communities, particularly men who have sex with men and trans people.
The importance of knowing your status
The 2023 FRA LGBTIQ III Survey introduced critical data on HIV testing, shedding light on disparities across sexual orientation, gender identity, and countries. Testing is a key step in ensuring early diagnosis and accessing treatment, yet the numbers reveal stark inequities:
- 47% of cis gay men had an HIV test in the past year, with peaks of 57% in Belgium.
- Among trans women, 43% reported testing, with rates as high as 57% in Cyprus.
- However, only 25% of gay trans men had tested in the last year, dropping to a concerning 2% in Hungary.
These figures show the urgent need for inclusive public health strategies and targeted funding programmes that dismantle barriers and encourage people across all LGBTI groups to access prevention, testing and treatment.
Breaking stigma, saving lives
Stigma and misinformation remain among the most significant challenges in addressing HIV. They discourage testing, silence conversations, and perpetuate discrimination. Yet, as Paul reminds us, activism rooted in personal experiences has the power to transform the narrative:
“I became a queer activist in large part because of my HIV status… I want to see a world ideally where HIV is history. We aren’t there yet, but I have confidence… that is an achievable goal.”
This World AIDS Day, let’s commit to empowering our communities with information, normalising discussions about HIV, and advocating for accessible, inclusive healthcare. Testing is not just a personal choice—it’s a collective step toward dismantling stigma and saving lives.
Take action
- Be informed: Know your status and encourage others to do the same.
- Be vocal: Challenge stigma and misinformation around HIV.
- Be engaged: Support LGBTI organisations advocating for HIV prevention and care.
Together, we can build a future where HIV is no longer a source of inequality but a chapter in history.
Trans and intersex rights at the forefront of positive change for LGBTI people in Europe, Rainbow Map finds
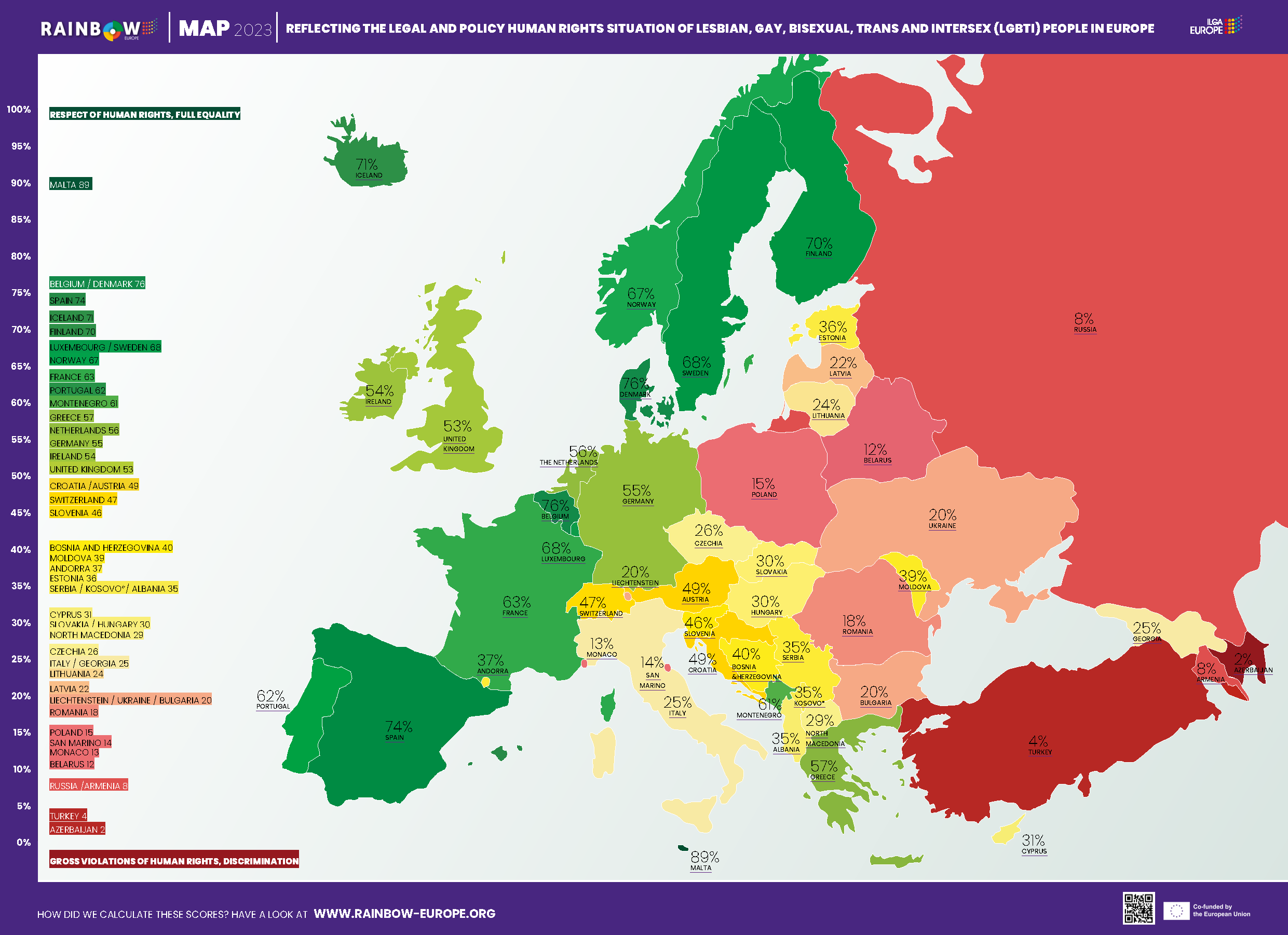
Despite intense anti-LGBTI attacks in several countries, equality is still advancing across Europe, ILGA-Europe’s annual Rainbow Map and Index shows.
The latest Rainbow Map and Index from Europe’s leading LGBTI organisation, ILGA-Europe, finds that while the public discourse is becoming more polarised and violent, particularly against trans people, political determination to advance LGBTI rights is paying off. The largest gains on the map are for countries that introduced legal gender recognition (LGR) using a self-determination model.
Published on Thursday, May 11, 2023 at the IDAHOT+ Forum in Iceland, ILGA-Europe’s annual Rainbow Europe Map and Index, ranking the legal and policy situation of LGBTI people in 49 European countries, finds that over the past 12 months bans on intersex genital mutilation (IGM) are also bringing countries up in the ranking. Spain jumped six places to number four with its introduction of LGR with self-determination, alongside a ban on IGM, while Finland entered the top ten, again up six places, again with LGR based on self-determination. Greece has also moved up four places with its ban on IGM.
Gender identity and sex characteristics are included in anti-discrimination and/or hate crime legislation, moving Belgium, Iceland and Moldova up the chart alongside Spain.
While the advancement of legislation recognising gender identity marks a major shift forward this year, there is more positive movement on the Rainbow Map and Index, notably:
- Moldova has jumped 14 places because sexual orientation and gender identity have been positively included in legislation covering employment, education, provision of goods and services, health, hate crime and hate speech.
- Slovenia and Switzerland switched positions. Both countries introduced same-sex marriage and joint adoption. Switzerland also allows medically assisted insemination for couples. Croatia too moved up one spot with its introduction of adoption for same-sex couples.
According to ILGA-Europe’s Executive Director, Evelyne Paradis: “As powerfully evidenced in this year’s Rainbow Map, the rise of anti-LGBTI rhetoric from anti-democratic forces, particularly instrumentalising false anti-trans narratives, is being fought back by politicians in Europe who have the courage to make a stand for the fundamental human rights and equality of every citizen. The map highlights the clear fact that progress for LGBTI people is still possible, and more important than ever, with the need for more leaders to push back on attacks on democracy for all by pushing forward. We commend those politicians who have taken the stance that needs to be taken for the good of everyone in our society, and we encourage more to step up to the plate as across Europe democracy and human rights are under threat from the far-right.”
Katrin Hugendubel, Advocacy Director at ILGA-Europe adds: “Governments, but also other political actors and institutions can and have been making a positive difference this year. A lot of progress relies on the Courts, for instance, at local, national and European level. Poland remains the country in the EU with the lowest ranking at 43rd place, but the country gained points in the index this year because of the courts ensuring that no surgical interventions are needed for legal gender recognition and the equality body extending its work to include intersex people. In a very hostile global climate, we are seeing different actors coming together, and weighing in more actively for LGBTI rights, which is crucial to counter the pushback.”
That pushback can also be seen in the challenge to freedom of assembly amid the rise of anti-democratic forces. Markedly, Serbia, which hosted a seriously compromised EuroPride march after last-minute attempts by the Serbian President and Minister of the Interior to ban the event, went down three places, while Turkey remains almost at the very bottom of the ranking after another year of crack-downs on Pride gatherings, showing that in 2023 the basic right to gather in a public space still cannot be taken for granted.
Released every May since 2009, marking International Day Against Homophobia, Transphobia, Biphobia, and Intersexphobia (IDAHOBIT), the ILGA-Europe Rainbow Map ranks all 49 European countries on a scale between 0% (gross violations of human rights, discrimination) and 100% (respect of human rights, full equality).
Executive summary 2023
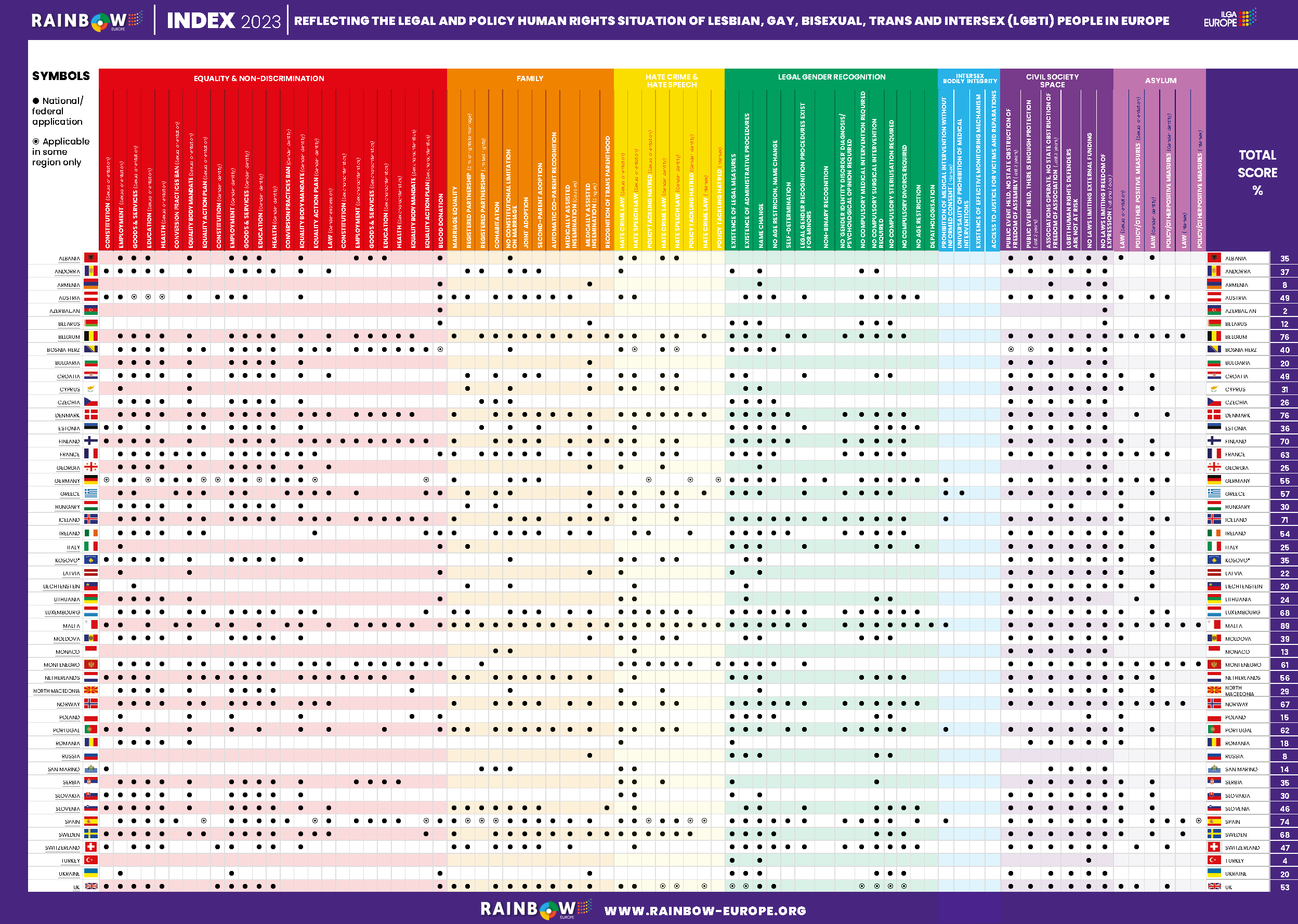
Rainbow Europe – ILGA-Europe’s annual benchmarking tool – comprises the Rainbow Map and Index and national recommendations. ILGA-Europe have produced the Rainbow Map and Index since 2009, using it to illustrate the legal and policy situation of LGBTI people in Europe.
The Rainbow Map and Index ranks 49 European countries on their respective legal and policy practices for LGBTI people, from 0-100%.
In order to create our country ranking, ILGA-Europe examine the laws and policies in 49 countries using 74 criteria, divided between seven thematic categories: equality and non-discrimination; family; hate crime and hate speech; legal gender recognition; intersex bodily integrity; civil society space; and asylum. More information on the list of criteria and their weight on the total score can be found at www.rainbow-europe.org/about
Policymakers, researchers and journalists are able to go ‘behind’ the points and see the original information sources that we base our Map and Index ranking on. This additional layer of information is available through our updated Rainbow Europe web module, www.rainbow-europe.org.
The Rainbow Map and Index presents a picture of what the policy landscape is like currently, while our country-specific recommendations attempt to answer the question “what’s next?” These recommendations are intended to encourage policymakers to address the most pressing legal and policy priorities within the framework of our Rainbow Map and Index.
The recommendations were gathered following an online consultation with a wide range of LGBTI organisations in the various countries. As a result, the recommendations are tailored to the needs of activists working on the ground.
- For the eighth year in a row, Malta continues to occupy the number one spot on the Rainbow Europe Map, with a score of 89%.
- With 76 points, Belgium now occupies the second place with a rise of four points due to the inclusion of gender identity and sex characteristics as aggravating factors in the country’s penal code.
- Denmark comes third place with a score of 76 with the rise of two points due to its new equality action plan, which includes specific measures on sexual orientation and gender identity but falls short of inclusion of projects on sex characteristics.
- The three countries at the other end of the Rainbow Europe scale are Azerbaijan (2%), Turkey (4%), and Armenia (9%), exactly the same as the last three years. Among them, only Armenia increased an index point after revoking its ban on blood donations from men who have sex with men.
- Spain, Iceland, Finland, Moldova, Switzerland, and Croatia are the countries with the biggest jump in scores. Spain introduced a comprehensive law that regulates legal gender recognition (LGR) based on self-determination, banned genital mutilations on intersex minors, prohibited so-called “conversion” practices and outlawed discrimination based on sexual orientation, gender identity, and sex characteristics.
- Iceland adopted an equality action plan, included gender identity and sex characteristics in their equality law, and added sex characteristics protection in the penal code. Moldova also amended its equality law and penal code to include sexual orientation and gender identity.
- Finland adopted its Trans Law which regulates LGR based on self-determination.
- Switzerland’s legislation on marriage equality came into effect, which also gave the right to joint adoption and medically assisted insemination for same-sex couples. In Croatia, same-sex couples can now apply for joint adoption and second-parent adoption after a court decision.
For further comment, contact: Ana Muñoz Padrós, ILGA-Europe: ana@ilga-europe.org, +32 493 35 60 55
Deadliest Rise in Anti-LGBTI Violence in Over a Decade, our annual Report Shows

12 years into annually reporting on the human rights situation of LGBTI people, Europe’s leading LGBTI equality organisation finds that pervasive hate speech across the region has led to life or death consequences.
Launched today in Brussels, ILGA-Europe’s Annual Review of the Human Rights Situation of LGBTI People in Europe and Central Asia finds that 2022 was the most violent year for LGBTI people across the region in the past decade, both through planned, ferocious attacks and through suicides in the wake of rising and widespread hate speech from politicians, religious leaders, right-wing organisations and media pundits.
This is the 12th edition of ILGA-Europe’s report, which has charted the growing phenomenon of anti-LGBTI speech, as antipathy for LGBTI people has been driven and then exploited for political gain. It finds that as a result, attacks on LGBTI people with a conscious and deliberate will to kill and injure have increased to unprecedented levels, including two terror attacks outside LGBTI bars in Norway and Slovakia, which combined killed four people and maimed 22. There are reports of more murders and many suicides of LGBTI people across Europe, and not only in countries that are seen to be more regressive.
According to ILGA-Europe’s Executive Director, Evelyne Paradis: “At ILGA-Europe, we have been saying for years now that hate speech in all its forms translates into actual physical violence. This year, we have seen that violence become increasingly planned and deadly, leaving LGBTI people feeling unsafe in countries across Europe. We have seen proof that anti-LGBTI hate speech is not just the words of marginal leaders or would-be autocrats, but a real problem with dire consequences for people and communities. This phenomenon is not only in countries where hate speech is rife, but also in countries where it is widely believed that LGBTI people are progressively accepted.”
The report finds that while hate speech and its consequences have reached critical levels, national and local courts are reacting and prosecutions are on the rise in several countries. But according to Paradis, reaction is not enough.
“While we are getting better at dealing with outcomes, the focus has to be on stopping hate speech in all its forms. Across Europe, many politicians have reacted with horror to the killings of LGBTI people this year, and while clear expressions of solidarity are always needed, it does not address the foundation of the problem, which is the proliferation of using hatred against LGBTI people for political gain. Our leaders need to find ways to proactively fight the rise of hate speech, rather than finding themselves in the position of reacting to its consequences.”
It is not all bad news. There has been much progress reported in several countries, with the Review consistently finding that it is activists and their communities who are driving positive social change and managing to push legal protection forward, despite organised opposition.
According to Katrin Hugendubel, Advocacy Director with ILGA-Europe: “LGBTI activists are the central players in countries where progress has been made, as we’ve seen in Spain and Finland, where huge effort went into successfully keeping self-determined legal gender recognition on the right political track, despite fierce opposition. This is true of every issue that affects LGBTI communities across the region, showing that LGBTI people and organisations remain empowered and continue to make change happen.”
The 12th ILGA-Europe Annual Review is available here, alongside all the previous Annual Reports, charting the phenomenon of rising anti-LGBTI hate speech in Europe and Central Asia, and its consequences.
According to Paradis: “These successive reports tell a story of cause and effect that is not going to go away or diminish until politicians and policy makers understand that they have to get ahead of the problem. In the current climate, progressive leaders must find effective ways to tackle hate speech in all its forms, instead of finding themselves on the back foot, expressing sympathy for the families of the needlessly murdered, or those who have taken their own lives, while hatred continues to be fostered and exploited.”
For further comment, contact: Ana Muñoz Padrós, ILGA-Europe: ana@ilga-europe.org, +32 493 35 60 55
Why cancer is disproportionally affecting LGBTI people

People are affected by cancer no matter what their identity is, but barriers in access to screening, prevention, and treatment puts LGBTI people at increased risk of developing fatal cancers. Keep reading to learn what can be done, so that no one is left behind in the fight against cancer.
Cancer is the second most common cause of death in Europe. With more than 3.7 million new cases every year, cancer prevention and screening programmes are crucial, yet LGBTI people are left lagging behind when it comes to this.
“The cancer community has recognised that the LGBTIQ+ community has historically been marginalised within the healthcare system, which translated into some discrimination, exclusion and unequal treatment in cancer care,” says Mike Morrissey, CEO of the European Cancer Organisation with whom we have been working together.
“This can often be caused by a lack of awareness of the specific needs of the community, policy guidelines that need updating to address the needs of marginalised communities, and the lack of inclusive language in both health documentation and medical check-ups, to name a few examples,” Morrissey adds.
Moving away from gendered language
Trans, intersex, non-binary and third gender people exist in Europe, but are left out when screening, prevention and treatment use binary categories to determine risk factors and eligibility. To put it more plainly, when your body doesn’t fit the binary boxes of ‘female’ or male’, this means that you may not receive the cancer care that your body needs.
Access to health services should be dictated by a person’s body parts and what their organs require to stay healthy. For example, when stating ‘women require mammograms’, we are leaving out those who are not women but are at the same risk of developing breast cancer. Moving away from gendered language in cancer prevention plans and instead referring to specific body parts, will ensure than trans, intersex, non-binary and third gender people can access to the screenings and treatment their bodies need.
Increased risk and lack of prevention for LGBTI people
Some studies suggest higher cancer rates for LGBTI people. While research into the reasons behind this greater prevalence is still too limited, we know that LGBTI people access routine healthcare less frequently than others. Some of the reasons are:
Fear of discrimination
Have you ever worried about talking about your sexual orientation, your sexual experiences, your gender identity, or your sex characteristics to your doctor because you are unsure if you will be treated the same way after you have shared this information? You are not alone. Fear of being discriminated against often prevents LGBTI people from sharing relevant information that could affect their health.
Limitations in access
Many LGBTI people encounter barriers in access to employment or education. These barriers prevent them from accessing healthcare too, and can prevent them having adequate health insurance coverage.
Negative experiences with healthcare providers
It is difficult to reach out to someone when you anticipate an uncomfortable time with them. Fear of having a negative experience with a healthcare provider can lead some LGBTI people to delay or avoid medical care, especially routine care such as screenings for early detection. Missing routine cancer screenings can lead to cancer being diagnosed at a later stage, when can be harder to treat.
Misinformation about cancer risks
Trans and intersex people in particular have historically been exposed to significant human rights violations in healthcare settings. For example, many trans and intersex people report non-consented or coerced gonadectomies wherein the “risk of cancer” was used as a motivator to encourage them or their parents to “consent” to the surgery. This brings further distrust of healthcare providers when it comes to discussions of cancer risks and treatments.
This is why any EU or national plans against cancer must ensure that LGBTI people will receive the screenings and treatments they need, when they need them, and with equal coverage under insurance schemes. As Mike Morrissey states, “the European Cancer Organisation could not achieve its mission to improve outcomes and quality of care for all cancer patients, if one specific marginalised community is not included in the advancements of the cancer community at large. It is therefore of utmost importance for us to bring together the cancer community and guide the effort in fighting for equity for all citizens and cancer patients regardless of their background.”
You can check out our latest feedback to the European Commission and more submissions to the EU Cancer Plan and the Cancer Screening Recommendation.
#WorldAIDSDay 2022: PrEP and Ending AIDS in the EU by 2030

EU countries have set 2030 as the target date to end AIDS in their populations. The provision of the HIV prevention medication, PrEP, is key to achieving this goal. However, half a million vulnerable people in the EU have no access to the drug. On World AIDS Day, we look at what governments need to do to make PrEP accessible for all.
Ending the AIDS epidemic by 2030 is the ambitious goal set by the United Nations eight years ago, to which EU countries committed along with many others. PrEP, or pre-exposure prophylaxis, is a vital component of this plan.
According to UNAIDS, 38.4 million people in the world were living with HIV in 2021. There 1.5 million new HIV infections last year and 650,000 deaths due to AIDS. In Europe and Central Asia, there is a persistent increase in annual HIV infections. Because it is highly effective in preventing infection, it is essential that PrEP is available for all those at risk. But the thorny truth is that this is far from the case.
Who can access PrEP? Who cannot?
Despite the efforts in the fight against AIDS, PrEP is still not accessible for many. In the EU, 500,000 gay, bisexual, and other men who have sex with men (MSM) who would like to take PrEP don’t have access to it. This represents a 17% gap, according to a 2019 study by the ECDC. The differences in price are also striking: generic PrEP can be found for €5 per month in some countries that include it in their national insurance coverage, while some brands cost up to €6,041 when national insurance does not provide coverage.
According to AIDS Action Europe, PrEP is more accessible in urban areas, information campaigns are often led by NGOs who might not have enough financial support, and as a result services and information target young educated gay, bisexual, and other MSM. Migrants, bisexual men, women (particularly women with migrant backgrounds), trans people and sex workers are left behind. Other populations at risk are people who inject drugs, prisoners and undocumented migrants, because they are not eligible for PrEP in many European countries, as reported by UNAIDS. So, what’s the way forward if the ambitious 2030 target is to be met?
The Top 6 Recommendations
Here are some key recommendations for governments in order to make PrEP available to everyone who might benefit from it, following the research by UNAIDS and AIDS Action Europe:
- Include PrEP as an HIV combination prevention
- Make the eligibility criteria more inclusive
- Develop awareness-raising campaigns that better target communities that are currently left behind
- Promote collaboration between communities and medical health providers
- Share experiences and best practices of implementation with those countries that have not implemented national PrEP guidelines yet
- Encourage strong data collection and add informal online access to PrEP and the relevant health outcomes to existing monitoring
For many years, ending AIDS in Europe was just a hope, but as time has gone on and medications have improved, this hope has turned into a real possibility. At ILGA-Europe, we will continue to work with governments and institutions to ensure equity in access to PrEP, as part of a whole package of measures to ensure the end of AIDS by the set target date.
Check out the Parliamentary Dialogue on Equitable Access to Oral PrEP within the EU and Beyond celebrated on November 25, 2022 to learn more.
Monkeypox: Why global equity must be central to contain the spread and how it can be achieved

Over 18,000 cases of monkeypox have been confirmed in the EU since the start of the outbreak in the region in May. Humanitarian organisations, governments and institutions must join forces and put equity at the centre of their thinking so treatments and prevention measures are available for all.
By the end of August, 18,072 confirmed cases of monkeypox have been reported from 29 EU/EEA countries, according to the ECDC, and 46 cases have been reported in the Western Balkans and Turkey. The first cases were registered in early May. Globally, over 48,000 cases have been confirmed since January 2022, according to WHO.
Who can get infected and how?
Monkeypox is transmitted by skin-to-skin contact of any kind, contact with contaminated clothing and fabrics, and by aerosol droplets; the current European and North American outbreak appears to be closely, though not exclusively, linked to sexual practices as well. There are right now specific outbreaks among men who have sex with men (MSM): over 95% of the reported cases in the world are linked to this practice.
Even so, anyone can contract the virus if they engage in risky practices with people who are potentially infected and sexual contact among men is not the only mode of transmission. The risk of infection comes from practices, not identities. This is important to keep in mind, not only to stay away from stigmatisation of gay and bisexual men communities but also to contain the spread, as we learnt from HIV/AIDS epidemic.
Are there vaccines and treatments?
The European Commission has secured 163,000 doses of vaccines to respond to the progression of the spread of this virus in the EU. Spain, Germany, Belgium, Sweden, Ireland and Italy are among the countries who have already received vaccines.
However, vaccines on their own are no silver bullet, says the WHO:
- 85% is the protection estimated from vaccines, according to the limited data available. Additionally, there is one single manufacturer authorised globally, which will probably mean shortages in supply.
- There are great disparities in distribution in the EU. In July, the European Commission announced an order for over 163,000 doses for all the EU, while countries like France had already purchased 250,000. Spain, with over 6,400 cases is the country with the highest number of cases in the EU, has had to this date only 17,000 doses available. These are examples of disparities in the distribution of vaccines in the EU, but as we learnt in 2020, a virus doesn’t know about borders.
- There are no vaccines at all in Africa. Still, the death-per-case rate in Central and Western Africa is 1 in every 21 cases, which is more than 100 times more than in the global north, less than 1 in every 2,500 cases.
What can institutions and governments do?
- Global public health is a global responsibility where equity is key. Vaccines and treatments must be made available in poor countries as well as in richer ones – this is the only way to ensure that outbreaks like this do not happen and that the virus does not become endemic. Therefore, the vaccine supply must be coordinated among countries and institutions such as the European Commission and the WHO.
- Vaccines are a preventative measure, not a reactionary one. Early diagnosis, contact tracing and exposure limitation measures must come along in order to ensure that the limited supply of vaccines has the largest possible impact.
- At a national level, ministries of health need to coordinate closely with LGBTI and HIV-related organisations to develop communications and outreach materials, as well as with groups organising events where transmission is likely so that they can communities with their communities effectively. In order to this, these groups and civil society must be granted sufficient resources.
- As with the HIV/AIDS epidemic, LGBTI civil society are taking up public health responsibilities to ensure that LGBTI people are effectively protected and served; however, this means diversion of resources from some of the core work of these organisations. Public health institutions must work in equitable, non-discriminatory ways to ensure services of the most vulnerable.
Joint statement on Protecting Abortion Access in Europe

AS the decision by the United States Supreme Court overturning Roe v. Wade, thereby dismantling the US constitutional right to abortion, ILGA-europe joins the center for reproductive rights, alongside many other organisations calling on european decision makers to remove impediments in access to abortion care.
The decision by the United States Supreme Court in Dobbs vs. Jackson Women’s Health Organisation overturns Roe v. Wade, thereby dismantling the US constitutional right to abortion. The decision will have a profound and devastating impact.
As local and global women’s rights, human rights and sexual and reproductive health and rights organisations working in Europe, we express our profound solidarity with the millions of people in the United States whose right to essential reproductive health care has been taken away by this decision and with all of those who have sought
to protect and uphold this right.
Keeping LGBTI people safe as the war in Ukraine continues

To mark IDAHOBIT on May 17, ILGA-Europe and UNAIDS, the Joint United Nations Programme on HIV/AIDS, will host an event focusing on the rights of LGBTIQ+ people in and from Ukraine. Here, our Executive Director, Evelyne Paradis speaks to UNAIDS about the particular challenges facing LGBTIQ+ people caught up in war.
Hi Evelyne, how do humanitarian crises particularly affect LGBTI people?
Humanitarian crises affect everybody, however, some communities sometimes need a targeted response because of pre-existing vulnerabilities. These particular vulnerabilities make people feel unsafe when dealing with humanitarian organisations providing safe shelter, basic necessities food and medical aid. Not knowing if they will be treated without discrimination, simply welcomed and be taken care of, is a barrier for people in accessing humanitarian support.
ILGA-Europe is heavily involved in the Ukraine crisis. What are the main challenges facing LGBTI people affected by the war?
In the Ukraine crisis, what we are seeing is that LGBTI people are not de facto integrated in first aid supply chains. Transition-related and intersex-specific medication, such as hormone replacement therapy, and to a certain extent medicines for people living with HIV, are not ensured in humanitarian packages at the moment. On top of this, a significant portion of the LGBTI community cannot meet their basic needs, due to pre-existing socioeconomic inequalities.
Trans women with a male gender marker on their documents can be obliged to join the army or cannot leave the country along with other women, which puts them in a potentially very harmful situation.
Having access to safe shelter is also an issue. In Ukraine, many LGBTI people don’t feel safe to be ‘out’ in regular shelter, while some who are displaced in the country are reporting facing discrimination when trying to rent an apartment. As a result many of the LGBTI groups have set up shelters to support their communities. Some of those who are staying and are visible have been physically attacked, as LGBTIphobia was already an issue in Ukraine before the war.
This is all happening while LGBTI people face the same struggles everyone else is facing; money, food, caring for loved ones, and so much more.
What are organizations like ILGA-Europe doing to help?
We are sending direct financial support to groups who are staying in Ukraine and are providing direct support to their communities, as well as to LGBTI groups in hosting countries. We’re also actively working to mobilise resources for all the LGBTI groups working in support of LGBTI people in Ukraine and abroad. We’re working with large humanitarian groups and organisations like UNAIDS and connecting them to the needs on the ground, while advocating with European institutions and governments to take action both in support of LGBTI communities in Ukraine and for LGBTI people who have left the country.
What can be done to better address the unique needs of LGBTIQ+ people in humanitarian crises?
What we are seeing is that an LGBTI perspective is really not integrated into humanitarian work and the development of protection measures, such as protection from gender-based violence or access to medicines. In many ways we have had to start from zero, including having to establish contacts with actors in the humanitarian sector.
While it is still early in this particular crisis to have specific recommendations, there will be no doubt be a lot of learning to be done from the work currently happening, so that we make sure that in future LGBTI perspectives and needs are integrated in the way humanitarian actors respond from the start.
Many civil society and community organizations are supporting LGBTI people affected by the war in Ukraine. What challenges do they face in carrying out this important work?
Most LGBTI organisations are not set up to be doing humanitarian work, and yet they are supporting basic needs in addition to the work they continue to do for their communities. But they cannot do it all. If they become the first point of support and assistance, there’s a lot of other work, like advocating for rights, that will not be done. This is true in Ukraine as well as in hosting countries.
Inequalities, stigma, discrimination and human rights violations against are continuing to prevent LGBTI people from being able to access the HIV and health services they need. How can we achieve positive political, legal and social change?
The work that has started with the humanitarian sector shows there’s a need, but it’s also an opportunity. If the humanitarian sector incorporates an LGBTI perspective and LGBTI people in their work from the start, this can mean a positive change for these communities, especially in times of crisis.
Register now for tomorrow’s event by ILGA-Europe and UNAIDS focusing on the rights of LGBTIQ+ people in and from Ukraine.
This interview was originally published on UNAIDS’ website.

IDAHOBIT 2022: Rights of LGBTQI+ people in and from Ukraine

On the occasion of IDAHOBIT, ilga-EUROPE and UNAIDS are hosting an event focusing on the rights of LGBTIQ+ people in and from Ukraine.
The event will take place on Tuesday, 17 May from 12:00 – 13:30 CET.
The interactive panel session will be moderated by Cianán Russell, ILGA-Europe’s Senior Policy Officer to discuss how to better protect the rights of LGBTIQ+ people in and from Ukraine.
The event will bring together:
- Victor Madrigal-Borloz, UN Independent Expert on sexual orientation and gender identity
- Olena Shevchenko, Representative of the Ukrainian LGBTIQ+ Community
- Tymur Lysenko, Representative of the Ukrainian LGBTIQ+ Community
- Matthew Kavanagh, UNAIDS Deputy Executive Director a.i.
- Marc Angel, Co-President of the European Parliamentary Intergroup on LGBTI rights
- Maria Arena, Chair of the European Parliament Subcommittee on Human Rights
- Katalin Cseh, Member of the European Parliament Committee on Foreign Affairs
- Joanna Darmanin, Head of Unit Humanitarian and Thematic Policies (C1), DG ECHO
- Kate Thomson, Head of Community Rights and Gender Department, The Global Fund
- Valeriia Rachynska, The Global Partnership to End HIV-Related Stigma and Discrimination
Briefing Document: Ukraine war – Medications needed by trans and intersex people
The ongoing crisis in Ukraine has resulted in need for immediate action to address the needs both of a significant population of Ukrainians fleeing the fighting as well as for those who are staying in Ukraine. Within both of these populations, trans and intersex people can be found, and their unique healthcare needs must be taken into account in the humanitarian responses. The purpose of this briefing is to describe the medical needs most common among trans and intersex people, including the medications that they will need, and to document emerging issues in Ukraine and surrounding countries on these issues.
Health
For more information contact: Cianán Russell, Senior Policy Officer
Part of the problem is that most policymakers and healthcare practitioners do not prioritise LGBTI-relevant health issues. A significant lack of systematic data only exacerbates this.
With that in mind, ILGA-Europe works towards securing effective legal protection for LGBTI people against any form of discrimination in the healthcare sector. Part of that task includes striving to strengthen European legislation and policies by building policy makers’ knowledge around LGBTI people’s health. We also work to prevent trans people from being psychopathologised because they are trans.
Together with our member organisations, who work on national levels, we identify good practices and try to operationalise them. We also support and assist with litigation cases in the European courts, and thoroughly collect data on discrimination and violence that LGBTI people face in healthcare settings.
To make an impact around all of those points, we embrace a number of strategies. For example, we support medical and ethical bodies in developing guidance and policies – and work to develop international human rights standards with the EU and Council of Europe. When violations happen, we ensure that they are well-documented by national and international bodies.
Overall, our work to improve LGBTI health centres around a few focus areas: equal access to healthcare, LGBTI health, HIV/AIDS and mental health. Across almost all focus areas, we collaborate with health-focused NGOs to ensure LGBTI awareness and inclusion, support national policy development processes and develop international human rights standards.
Here is how we work with each of these focus areas:
Equal access to healthcare
Equal access to healthcare includes advocating for thorough data collection about the discrimination and violence that LGBTI people face in healthcare settings. It also entails adequately training healthcare providers and medical students to prioritise LGBTI-relevant care.
At ILGA-Europe, we specifically work to ensure equal access to healthcare by developing and disseminating inclusive, human rights-based healthcare training materials.
LGBTI health
When we talk about LGBTI health, we mean advocating for a few things. First of all, we demand full implementation of the International Classification of Diseases, 11th Revision (ICD-11). We also advocate for healthcare practitioners to have access to and awareness around human rights-based medical guidelines, medical education and standards of care. Last but not least, we work to increase funding to LGBTI-specific healthcare projects.
How do we do this? In short, we provide support across all those points – from ICD-11 implementation to the creation of human rights-based medical guidelines.
HIV and AIDS
Across Europe, HIV transmission rates among men who have sex with men (MSM) and trans people (trans women in particular) remains high. Diverse factors explain why – like ongoing discrimination and stigma against LGBTI people, which can lead to low self-esteem and late diagnoses. Moreover, sexual and relationship education for young people across Europe is subpar – which poses a major problem to effectively tackling HIV.
With that in mind, ILGA-Europe advocates for LGBTI-relevant healthcare programming to combat the HIV and AIDS epidemic – with a focus on the most marginalised groups. We also work to secure funding for inclusive programming from sustainable government sources, and to disaggregate data on the grounds of SOGIESC.
Primarily, we do this by collaborating with health-focused NGOs to ensure LGBTI awareness and inclusion – and by developing relevant messaging. We also participate in the Nobody Left Outside initiative and support national policy development processes.
Mental health
Stigma and discrimination negatively impact LGBTI people’s mental health. This is illustrated by the concept of ‘minority stress’ – a psychological distress that comes from experiences of marginalisation, discrimination and stigmatisation. Minority stress can lead to increased risk of suicidal behaviour, self-harm or depression.
To ensure better mental health for LGBTI people, ILGA-Europe advocates for including LGBTI-specific issues in mental health law and policy. We also advocate for disaggregating data on the grounds of SOGIESC.
On a practical level, we work towards these goals by collaborating with NGOs focusing on mental health to ensure LGBTI awareness and inclusion in their programming and work. We also promote our members’ work around LGBTI mental health.
Subscribe for more info on this topic
LAW / POLICY PAPERS / REPORTS


Trans Day of Visibility 2022: Here’s what you absolutely should know about trans communities from Ukraine

It’s March 31, Trans Day of Visibility. To mark this day, at ILGA-Europe we want to commend the amazing work trans-led organisations are doing as the war in Ukraine continues, and tell you about the current needs of trans communities staying or leaving the country.
After over a month of war, Putin’s invasion of Ukraine has devastated several cities and caused the displacement of almost four million people and counting. Trans people are among those affected: there are trans women who have tried to leave but couldn’t due to the male gender marker in their passports, and trans people who want to stay but are at risk of violence in regular shelters, and all are exposed to potential shortages or difficulties in accessing medicines and hormones on both sides of the border.
Trans-led groups and organisations are responding to the humanitarian crisis by doing an incredible job to support trans people in Ukraine and neighbouring countries. Here are some of the current needs of trans people from Ukraine and how trans-led organisations are responding:
Trans people staying in Ukraine or leaving — what are their needs?
- Many trans people in Ukraine do not have identification documents with gender markers matching their gender identity. So trans women often still have a male gender marker. In this situation, many of those who have tried to flee have been refused to pass internal check-points and to leave the country as due to their identity documents, they fall under the martial law and military mobilisation of men between 18–60. Trans women need a pathway to be able to leave the country along with other women, including those who have a male gender marker in their documents.
- Trans people and other LGBTI communities who are staying in Ukraine because they want to, or because they cannot leave, are at risk of discrimination and violence in regular shelters. The few existing LGBTI shelters have very little capacity.
- Necessary hormones and medicines for trans and intersex people, as well as HIV/AIDS medication are, like other supplies, running out in Ukraine. Humanitarian aid packages generally do not include these medicines, and trans, intersex, and LGBTI civil society groups in neighbouring countries are working hard to fill this gap in the short-term. It is imperative that medicines are available for trans communities in Ukraine and for refugees in arrival countries.
- When trans refugees arrive in neighbouring and other reception countries, many may experience delays and inconsistencies in access to healthcare, which could lead to an interruption in their care. This can be potentially devastating. Governments in reception countries must enable access to healthcare for refugees and ensure that trans and intersex people already taking medicines can continue care without interruption.

Many trans-led organisations are doing amazing work to help and support their community members from Ukraine. Have a look:
In Europe, TGEU is monitoring the situation, providing frequent updates and resources, as well as how best to provide support, guidance for trans people from Ukraine, and visuals for social media channels, here.
In Ukraine and Slovakia, Trans*Generation is providing legal consultation and connections to trans people who want to cross the border, as well as information about visas abroad, hormones and medication and financial assistance to trans people staying and leaving Ukraine. Find out more here.
In Hungary, Transvanilla is supporting trans refugees crossing the border by providing transport, accomodation, translation and accompaniment in administrative procedures. Learn more about Transvanilla here.
In Poland, intersex organisation Fundacja Interakcja is supporting trans and intersex refugees. Learn more here.
Behind the smokescreen of anti-LGBTI rhetoric in Europe, there’s a groundswell of allied determination to tackle hatred, report finds
A report from the leading LGBTI organisation in Europe finds that amid a rise in official anti-LGBTI rhetoric fueling a wave of hate crime in every country in Europe, there is a growing institutional resolve to tackle hatred and exclusion.
Published today, February 15, 2022, ILGA-Europe’s Annual Review of the Human Rights Situation of LGBTI people in Europe and Central Asia finds that while there was a staggering rise in 2021 of anti-LGBTI rhetoric from politicians and other leaders, fuelling a wave of violence, with anti-LGBTI hate crime reported in every country, the response to this has been an allied determination in many countries, and at the European level, to tackle hatred and exclusion of LGBTI people.
Politicians in countries across Europe, not just in the usually reported Hungary and Poland, have continued to demonise LGBTI people over the past year, leading to a stark rise in anti-LGBTI attacks, burning of rainbow flags, and targeting of young LGBTI people in particular. A particular low point of the year came on June 15, with Hungary’s introduction of legislation which introduced a ban on the “portrayal and the promotion of gender identity different from sex at birth, the change of sex and homosexuality” for persons under 18.
Reported violence against LGBTI people in this context across Europe was rife. Germany, for instance, had a 39% increase in anti-LGBTI hate crime, while a new app in France, where users can report anti-LGBTI hate crimes, collected reports of 3,896 incidents in its first year. In the second year of the COVID-19 pandemic, domestic violence against LGBTI family members continued to take place widely. There were murders, assaults, corrective rapes, and anti-LGBTI police brutality. In many countries where police brutality took place, the police were not held accountable.
Anti-gender and anti-trans rhetoric have remained widespread, often targeting youth in particular. The narrative pitching trans rights against women’s rights also continued apace this year, and in this context there was stagnation in legal gender recognition (LGR) reform in many countries.
According to Executive Director of ILGA-Europe, Evelyne Paradis: “The spread of anti-LGBTI and trans exclusionary rhetoric outlined in this report has a very real negative impact on people’s lives. In country after country, we see how it negatively impacts people’s mental health and their sense of safety, their access to employment and the overall ability to progress much needed legal protection. At this moment in time, it is essential we remind politicians, media, academics – and sadly even some civil society actors – that real people’s lives are at stake in every country across the region, because of the political scapegoating of LGBTI people.”
In the context of this political scapegoating, national human rights institutions (NHRIs) and courts in many countries have begun to strengthen their work to protect the rights of LGBTI people. The European Court of Human Rights delivered several positive judgments this year, on hate crimes, freedom of assembly, LGR and family rights.
By far the strongest commitment to LGBTI human rights from European Union level came when the European Commission (EC) in July opened landmark infringement procedures against both Hungary and Poland. The European Parliament also adopted its resolution on LGBTIQ rights in the EU, strongly supporting the EC’s objective to propose legislation in several areas of protecting LGBTI rights, and condemning where member states have not been respecting EU law as regards LGBTI rights.
Said Katrin Hugendubel, Advocacy Director at ILGA-Europe, “This report narrates an unparalleled year in Europe, with regional and national institutions and courts taking their obligations to the human rights of LGBTI people with utmost gravity amid the now crystal clear escalation of the instrumentalisation of hatred against LGBTI people for political gain and expanded power. The advance of using hatred of any minority as an instrument of political gain, which we have seen throughout history, must be addressed and halted with allied determination across the region.”
It is also clear from this report that state-sponsored anti-LGBTI rhetoric and legislation is not matched by public opinion. Support for LGBTI people has never been stronger. In Hungary, for instance, a representative poll commissioned by Amnesty International Hungary and Háttér Society and conducted by polling agency Medián between 13 and 19 July 2021, found that 73% of Hungarians reject the government’s false claim that gay and lesbian people abuse or harm children.
A clear majority of Hungarian society (74,5%) believe that transgender people should be able to change their gender and name in their official document, while 59% support same-sex marriage. Hardly any Serbians know trans people, but 60% think they should be protected from discrimination. 68% of Romanians think all families, including rainbow families, should be protected, while 40% of Bulgarians would support a party that is pro-LGBTI.
According to Soudeh Rad, co-chair of the ILGA-Europe board: “While these numbers and outcomes of similar polls are promising as heartwarming illustrations of the strength and impact of the work carried out by civil society and the LGBTI movement at global, regional, and local levels, we must not forget the struggles activists across Europe and Central Asia face in realising a world where everyone can enjoy their human right to fully be themselves.”
Check out our Annual Review 2022.
Navigate the Annual Review chapters by country, institution or theme at our Rainbow Europe module!
For further comment, please contact ILGA-Europe’s Communications and Media Officer Ana Muñoz Padrós at ana@ilga-europe.org or +32 493356055.
Annual Review 2022
The Human Rights Situation of Lesbian, Gay, Bisexual, Trans and Intersex People in Europe and Central Asia between January-December 2021.
The Annual Review is ILGA-Europe’s annual publication documenting legal, political and social developments in 54 countries and 4 European institutions over the past calendar year. It is a unique report tracking key positive and negative trends in relation to LGBTI equality and human rights in Europe and Central Asia.
This year’s review finds that behind the smokescreen of anti-LGBTI rhetoric in Europe, there’s a groundswell of allied determination to tackle hatred.
Check out other editions

The Frontline: The LGBTI Activist Wellbeing Challenge

While a number organisations and groups have already taken concrete steps to address wellbeing, there’s no golden rule on how to approach these challenges. In this episode we share what ILGA-Europe has been doing to support the wellbeing of the movement.
Joining us to talk about the distinctive approaches they’ve used to tackle wellbeing issues for their teams are David Kakhaberi, the executive director of Equality Movement in Georgia, and Eka Tseriteli, executive director of Women’s Initiatives Supporting Group, also in Georgia.
Listen below or click here to listen and subscribe to The Frontline on your favourite podcast platform.
Why knowing your HIV status is good for your health and wellbeing

For different reasons, many sexually active people don’t want to know whether they are HIV positive or not. They don’t want to even think about it. But if you do know what your status is, one way or the other, you will be making a positive difference to your life. Here’s why…
Do you know your HIV status? According to the World Health Organisation (WHO), over half a million people in Europe don’t know they are living with human immunodeficiency virus or HIV. Many of them are still afraid to get tested because of fear of prejudice and discrimination against people living with HIV and AIDS. LGBTI people who are HIV positive often face a ‘double stigma’, including within their own communities.
But a better quality of life for people living with HIV and AIDS depends on testing. Only after knowing their status, can HIV positive people start a treatment, and obtain support and social protection. In advance of World AIDS Day, we have joined the European Testing Week to encourage people to get tested on HIV and hepatitis. Although there is no cure for HIV yet, treatments can enable a greater life expectancy and prevent the transmission of the virus to others.
Testing is the first step to greater life expectancy for people living with HIV. As the virus attacks the immune system, a person with HIV is at risk of developing serious infections. The ability to fight other diseases like cancer weakens too. But if you know you are HIV positive, and access treatment, you can help prevent the development of other infections and increase your ability to fight disease.
Testing and following treatment also limits the risk of passing the virus to someone else. Today, there is scientific evidence proving that undetectable equals untransmittable (U = U). This means that people living with HIV who achieve an undetectable amount of HIV in the blood by taking antiretroviral therapy cannot sexually transmit the virus to others. Therefore, testing is not only important for your own health and wellbeing, but also for others.
How HIV tests work?
The most common form of HIV test is a blood test and today it can provide an accurate status within a month of infection. The blood is tested several times before someone is given a positive result. In some countries, saliva tests and dried blood tests are also available; these tests provide a rapid accurate result, but are a bit less able to detect very recent infections. Voluntarism, privacy and confidentiality should be assured and respected while getting tested.
How is HIV transmitted?
- HIV is transmitted through contact with blood, sexual fluids and breast milk
- The main routes of transmission are through unprotected sex and by sharing injecting equipment
Where to get tested?
EuroTest has put together a list of places where you can access a HIV test:
- Sexual health clinics, also called genitourinary medicine (GUM) clinics
- Hospitals, department of infectious diseases
- Clinics or testing sites run by community based HIV/hepatitis organisations or charities
- Some General Practitioner (GP) surgeries and GPs
- Some contraception and young people’s clinics
- Local drugs agencies
- Antenatal clinics, if you are pregnant
- Private clinics
Check out the NAM European test finder to find a testing centre near you.
Help moving forward, if you test positive
If you have tested positive for HIV you may feel overwhelmed at the moment, and that’s okay. Solid communities and organisations’ networks across the world are there to support you whenever you need so. To seek treatment and care, EuroTest recommends these websites:
Mental Health: Dealing With Stress as an LGBTI activist

2020 has drastically altered our daily lives and as an activist it’s easy to put your mental health and wellbeing on the back burner, while you get on with other hugely pressing priorities. On top of this, LGBTI activists can suffer from particular mental health stresses that stream from discrimination, LGBTIphobia, and the uphill battle that working to secure our rights and equality can be. To mark World Mental Health Day, this blog brings you some tools to help you cope with challenges that come your way.
“A field that has rested gives a beautiful crop.” — Ovid
It’s been a remarkably arduous year for all of us on a global level, and considering that LGBTI communities can carry additional burdens, it’s especially important to take care of our mental health and wellbeing. Mental health, as defined by the World Health Organisation (WHO), is a state of well-being in which an individual realises their own abilities, can cope with the normal stresses of life, can work productively, and is able to make a contribution to their community. We can think that because we don’t have a particular mental health condition, that we are fine, but mental health is more than the absence of mental disorders.
The particular stresses on LGBTI activists
Stress is a totally natural reaction — it is the way our bodies respond to challenges in our environment. Having a certain amount of stress is positive as it can improve our motivation and effectiveness. Yet, intense and prolonged stressful situations affect our wellbeing. Here are some particular stresses that LGBTI activists face every day.
- Facing LGBTIphobia in both real life situations and on a daily informational basis
- Being overwhelmed by perceived and real barriers to positive change
- Being overwhelmed by negative news
- Being overwhelmed by too much work, often with no financial compensation
- Being overwhelmed by the perceived and real expectations of the community
Stress affects our body (physical reactions), it influences our mood (emotional responses), and it changes our behaviour. In the table below are the examples of different types of reactions that may arise.

How to effectively deal with stress
There is no universal solution to deal with stress, because:
- Stress is person specific — what stresses one person may not stress another person in a similar situation.
- Stress is time specific — what may stress one person at one point in time, it may not stress them at another time, sometimes because their experience mitigates it or the stress has become cumulative.
- Stress is context specific — having similar experiences in different contexts, for example, a context where you count on supportive relationships while another where you don’t, can fundamentally shift the experience of stress.
So, it stands to reason that dealing with stress is an individual thing. We need to identify the key factors of why and how we get stressed, and look at ways of changing them. For instance, how do you take care of your stress levels when going into a particular situation, say one of conflict with an anti-LGBTI group? What are the things you can put in place for yourself to manage the stress in that moment, such as breathing consciously or repeating a calming mantra in your mind? What are the ways your work as an LGBTI activist gets you stressed? If for instance, you can become overwhelmed by how much you are needed, how do you find ways to disengage for a moment so that you can tune into your stress levels? What are the self-compassionate breaks you can put in place for yourself on a daily basis that take you away from being overwhelmed? Activism is based in compassion for the human race, and you are part of that, so you need to be compassionate towards yourself as you do this work.
Stress is individually experienced, based on our own personalities and circumstances, but here are five universal elements for coping with stress in your daily life:
- Check how stressed you are: are there some signs of stress mentioned in the table above?
- Identify what is causing your stress — observe your daily routine and identify the triggers. It is important to know what is causing stress.
- Take care of the basics — try to eat healthy food, do some physical exercises, and have proper sleep.
- Make sure there is space in your daily routine for pleasant things: a walk in the park, a chat with a friend, cooking a meal — anything what brings you positive feelings.
- Talk to other people about your stress and ways to relieve it. You can talk to people you trust (friends, colleagues etc.) or you can appeal to the help of specialists / coaches / consultants. Currently there are plenty of people and organisations offering professional help on burn-out prevention.
What we can learn from 15 brave stories of real European intersex lives

“Sometimes it is necessary to speak clearly from a very personal or intimate point of view,” says intersex activist Ins A Kromminga, co-founder of OII Europe and illustrator of ‘#MyIntersexStory: Personal accounts by intersex people living in Europe’. The 15 beautifully illustrated, but often harrowing stories in this groundbreaking publication speak “a clear and frank language of things that are often hard to speak about”.
For intersex people, whose bodies are all too frequently referred to only in medical terms, there is great power in being able to tell their stories in their own words. This was one of the aims of ‘#MyIntersexStory: Personal accounts by intersex people living in Europe’, a book with 15 frank and unflinching testimonials, published this year by OII Europe.
Based in Berlin, OII Europe is the umbrella organisation of European human rights-based intersex organisations. It works for the full implementation of human rights, bodily integrity and self-determination for intersex people and is a member organisation of ILGA-Europe.
The illustrations by Ins A Kromminga in ‘#MyIntersexStory’ portray people who could be your neighbour, your friend, your co-worker, while at the same time showing that intersex people are resilient, strong and beautiful.
At the same time, the drawings are illustrative of a huge issue for intersex people that still remains over a quarter of a century since the first historic demonstration by intersex activists. Find out how in this powerful interview.
Hi, Ins. To begin with, tell us how the #MyIntersexStory project began?
The original idea came from a brochure we created within a project of a local and national organisation in Germany, at the time when the first study on feminising and masculinising surgeries on intersex children of the age 0–9 was published. The study showed that these intersex genital mutilations (IGM’s) continued, despite other claims from the medical field. We wanted to provide an additional resource to give the statistics in the study a human and relatable perspective.
In the brochure we deliberately refrained from reproducing medical and diagnostic descriptions to explain certain operations and diagnoses, and instead have intersex people describe what happened to them in their own words. The brochure contained short quotes by intersex people and their experiences of how the medicalisation had affected, and continued to affect, their lives, combined with colourful graphic representations of individuals in everyday situations.
The German brochure initialised the idea for a similar publication in English with a European scope of testimonials, which would include artwork that visually corresponded with the stories.

How did you creatively experience the process of illustrating such incredibly personal stories?
The process took quite a long time and changed several times in terms of how to approach the testimonials from an artistic standpoint. The project grew bigger over a period of almost three years of developing and finishing the final book. We included additional testimonials, and the images became much more intricate than originally intended.
The people who contributed to this project are incredibly brave and we thank each and every one of them for agreeing to share their stories. Without their willingness to put those stories on paper — which also includes reliving the experience of IGM to a certain extent — this book would not have been possible.
As an intersex activist and as a professionally trained visual artist, these two aspects in my life always competed with each other for time and attention, and the best moments for me are when I can combine the two. This was the case when I created the images for ‘#MyIntersexStory’. As I point out in the introduction, I did not want to ‘illustrate’ one specific person or story, but instead have the images show people who could be anyone in our society — a neighbour, a family member, an old friend from school. I also wanted to show that intersex people are resilient, strong and beautiful.
At the same time, and in a more subtle way, using illustrations also shows a remaining big issue for intersex people. The majority still live in the closet and are afraid (often with good reason) to show their faces and speak up in a society that continues to discriminate and pathologise intersex realities, and where legal protection is non-existent in most countries.
That’s why not one person in the images and stories is recognisable or identifiable. The personal accounts speak a clear and frank language of things that are often hard to talk about. They are very personal and subjective, but, as in the text in the book by Janik Bastien Charlebois points out, they are the forefront of intersex activism and precious and valuable forces in our fight for dignity.
I did not want to ‘illustrate’ one specific person or story, but instead have the images show people who could be anyone in our society — a neighbour, a family member, an old friend from school. I also wanted to show that intersex people are resilient, strong and beautiful.
Ins A Kromminga
In the introduction you write about stepping “out of invisibility”, but also “deciding on what and how much we want to share”. What obstacles does the intersex community face in finding the right balance between telling and keeping boundaries, which other communities may not face?
To share one’s personal account of being intersex can be difficult. There continues to be many misconceptions on what the term intersex means and who the people behind that word really are. And when people learn of the many ways one can be intersex, it quickly can become overwhelmingly complex, and at the same time boringly normal.
Since the issues intersex people experience often have to do with how our bodies are perceived by others, specifically the medicalisation of our variations of sex characteristics and the human rights violations they entail, things get very personal and private quickly. Therefore, as intersex activists we have developed a sensitive language to speak about our experiences without disclosing aspects that should remain every person’s individual choice to reveal. Sometimes it is necessary to speak clearly from a very personal or intimate point of view, but how much, or in what depth, everyone needs to decide for themselves, depending on the context. For example, I would speak differently with a close friend or partner about things than I would on a public panel.
Most of us have experienced such an intense level of taboo and stigmatisation, often from a very early age, that coming out can feel like liberation from a heavy blanket of silence and invisibility. The sheer need to communicate and put into words what otherwise had no concept or language, can lead to an urge to not holding back any details, in ways that might not always be good for ourselves or others. As intersex people we have to carefully re-learn what is necessary to talk about, and how much we want, or have to, share with the world.
Is the personal political?
Yes. Longer answer: the phrase that stems from the feminist and radical feminist movements is also true for intersex people. Fragmented and isolated under a medically prescribed taboo and the stigmatisation of bodily difference, every individual intersex person has to first do the archeology of their own story that lies buried under disinformation and silence.
The second step to realise that this very personal experience was not indeed as individual as it initially might have seemed, but instead is part of a systemic medical protocol that had spread globally by the end of the 1960’s. Intersex variations are still considered a disorder of sex development in the newest edition of the International Classification of Diseases (ICD-11), even though over 70 United Nation Treaty Bodies and many other human rights institutions have clearly identified and condemned the human rights violations and abuses intersex people face in most countries, which often happen within medical settings.
Intersex bodies, similarly to women’s bodies or the bodies of people with disabilities have been historically medicalised, objectified, ostracised and marginalised. We are all survivors of a heterosexist and patriarchial system that still does not want to loosen its grip and reflect and share the world with all human beings.
Fragmented and isolated under a medically prescribed taboo and the stigmatisation of bodily difference, every individual intersex person has to first do the archeology of their own story that lies buried under disinformation and silence.
What social change can be achieved through art and personal stories that cannot be achieved through advocacy work?
In the end we want to change our societies so that intersex people can enjoy their human rights just as every other person should be able to. In order to get there, there are many ways to inform, educate, raise awareness, advocate, consult and engage, and OII Europe believes in the benefit of using them in all their diversity.
In our eyes art and personal stories open other additional channels of empathy; they make people understand or relate on a more direct and emotional level. I think we will always need both, advocacy and legislation that will protect the rights of people, but also a change in culture, also through art, that speaks about the core of what it means to be human and how intersex people are part of humanity and our societies.
Some of the protagonists of the book are over 30, 40 and 50 and had surgical intervention when they were babies or children. Have the protocols in European health systems got better ever since? What has changed — or has not — for that to happen?
Since the first intersex people rallied in front of a medical conference in Boston 24 years ago, the medical field has adjusted and changed its approaches. Unfortunately their adjustments, with a few exceptions, mainly focus on reframing the issue and changing terminologies, not stopping the interventions of unconsented cosmetic surgeries and other medical treatments, as recent studies from Germany show.
Those interventions are often based on social constructs and biases. Regarding people born with variations of sex characteristics, the sole reason non-vital medical interventions, i.e. cosmetic feminising and masculinising operations, are performed is to make us look and function as (heterosexual) boys and girls, and later as men and women who will engage in heterosexual classical penetrative (penis-in-vagina) intercourse.
That this is not working should be clear after almost 30 years of criticism by intersex activists. The norm of the heterosexual and sex-binary human is one we have to overcome. Our world is much more colourful and diverse, and we all need to cherish it, not fear or regulate it.

Some words that are repeated across the 15 stories are very strong: “object of science”, “lack of information”, “medical violence”, “mutilation”, “body betrayal”. What words would you like to be shared by the intersex community instead of these?
Integrity, dignity, truth, intact intersex generations, autonomy, decency, informed choice, intersex-centered health care, celebrating diversity, intersex is beautiful, loving our bodies, exploring our full potentials, hermpower, hermlove, hermhugs, too cute to be binary… I shall collect more of those!
How did you first get involved with OII Europe?
I am one of the co-founders of OII Europe, which was founded during the Second International Intersex Forum in Stockholm, Sweden on Human Rights Day 2012 (December 10) as a network of national European intersex-led organisations. After our official founding as a charitable non-profit organisation in 2015, I served as part of the executive board for several years. I have been a member of the staff since January 2019, working as the Awareness Raising & Campaigns Officer, where I can integrate both my activist and artistic backgrounds.
What are the goals of OII Europe in the short and mid-term?
Our main goals are based on the Malta Declaration, formulated at the 3rd International Intersex Forum 2013. We work for the full implementation of human rights, bodily integrity and self-determination for intersex people, and the main short-term goal would be the legal prohibition of non-consensual medical and psychological treatment.
Something we already work on, but which could be considered ongoing or a mid-term goal, is the promotion of self-awareness, visibility and recognition of intersex people and for the full protection against discrimination and the adoption of “sex characteristics” as a protective ground.
In general we are working on supporting and informing stakeholders, multipliers, allies and educating the society at large on intersex issues from a human rights perspective.